


ýä£ Ùíá
ýêÿýï¡ Ùàä ÙÅÖýòê ýòö ý╣ÿÙúîýØÿ Û©░ý┤êÙèö ýêÿýêá, ÝÖöÝòÖ ýÜöÙ▓ò Ù░Å Ù░®ýé¼ýäá ýÜöÙ▓òýØ┤ýùêÙïñ. ÝòÿýºÇÙºî ýºÇÙé£ 10ÙàäÛ░ä ýâêÙí£ýÜ┤ Û░£ÙàÉýØÿ ý╣ÿÙúîÙ▓òýØ┤ ýòö ý╣ÿÙúîýØÿ ÛÀ©Ùª╝ýØä Ù░öÛ¥©Û│á ý×êý£╝Ù®░, ÛÀ©ýñæ Ù®┤ýù¡ ý╣ÿÙúî(immunotherapy; ýòöýØä Û│ÁÛ▓®ÝòÿÙèö ÝÖÿý×ÉýØÿ Ù®┤ýù¡ ý▓┤Û│äýØÿ Ý×ÿýØä ÙÅÖýøÉÝòÿÛ│á Û░òÝÖöÝòÿÙèö ýÜöÙ▓ò)Û░Ç ýù¼Ùƒ¼ Û░ÇýºÇ ýòöýóàýùÉýä£ Ýæ£ýñÇ ý╣ÿÙúîÙ▓òý£╝Ùí£ ý×ÉÙª¼ ý×íýòÿÙïñ[1]. CAR-T ýä©Ýż ý╣ÿÙúîýᣠÙÿÉÝò£ Ù®┤ýù¡ ý╣ÿÙúî ýñæ ÝòÿÙéÿÙí£ 2017ÙàäÙÂÇÝä░ 6Û░£ýØÿ ý╣ÿÙúîýá£Û░Ç Ù»©ÛÁ¡ Food and Drug Administration (USFDA) ýè╣ýØ©ýØä Ù░øýòä ýé¼ýÜ® ýñæýØ┤Ùïñ(Table 1) [2-8].
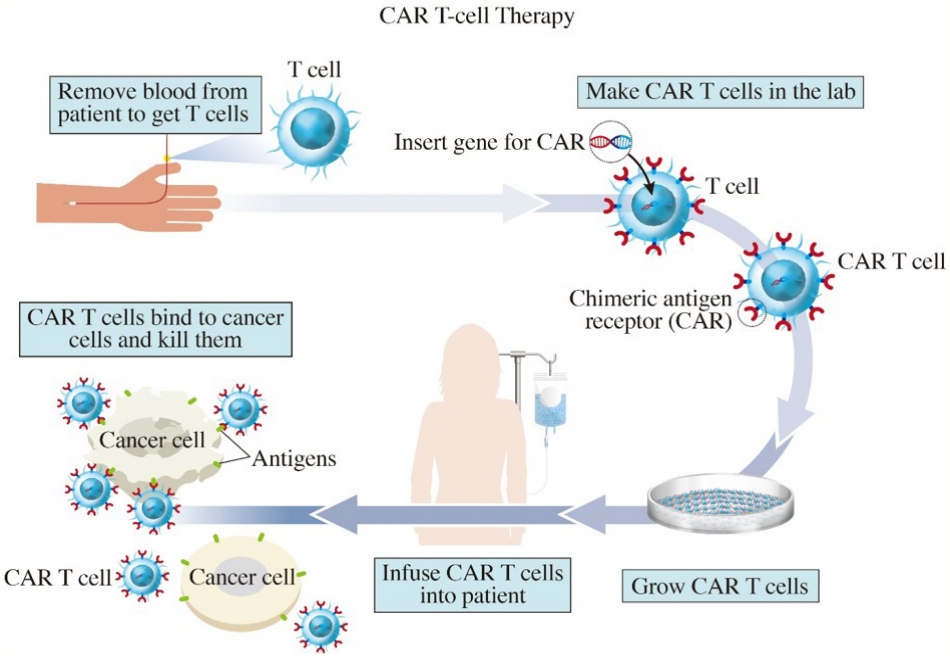
CAR-TÙèö ÝÖÿý×ÉýØÿ ÝÿêýòíýùÉýä£ Týä©ÝżÙÑ╝ Ù¢æýòä ýòöýä©ÝżÙÑ╝ ý×ÿ ýØ©ýïØÝòá ýêÿ ý×êÙÅäÙíØ ý£áýáäý×É ýí░ý×æýØä Û▒░ý╣£ ÙÆñ Ù░░ýûæÝòÿýù¼ Ùïñýï£ ÝÖÿý×ÉýØÿ Ù¬©ýùÉ Ýê¼ýò¢ÝòÿÙèö Û░£ýØ© Ùº×ýÂñÝÿò ýØÿýò¢ÝÆêýØ┤Ùïñ(Fig. 1). ýØ╝Ù░ÿýáüý£╝Ùí£ ýä©Ýż Ù®┤ýù¡Û│äÙèö ýêÿýºÇýâüýä©ÝżÙÑ╝ ÝåÁÝò┤ Û░ÇÛ│ÁÙÉ£ Ýò¡ýøÉýØä Týä©ÝżÛ░Ç Týä©Ýż ýêÿýÜ®ý▓┤(T cell receptor, TCR)ÙÑ╝ ÝåÁÝò┤ ýØ©ýïØÝòÿýù¼ ÝÖ£ýä▒ÝÖöÙÉÿÙèö Ù│Áý×íÝò£ Ù░®ýïØý£╝Ùí£ ý×æÙÅÖÝò£Ùïñ. ýØ┤ýÖÇÙèö Ùï¼Ùª¼ CAR-TÙèö Ýæ£Ù®┤ Ýò¡ýøÉýØä ý×ÿ ýØ©ýïØÝò£ÙïñÛ│á ýòîÙáñýºä Ýò¡ý▓┤ÙÑ╝ ýé¼ýÜ®ÝòÿÙèö Ù░®Ù▓òýØä ýô░Û▓î ÙÉÿÙèöÙì░, Týä©ÝżÙèö ýóàýûæýØä ýØ©ýïØÝòÿÙèö Ùì░ Ýò¡ý▓┤ÙÑ╝ ýé¼ýÜ®ÝòÿýºÇ ýòèÛ©░ ÙòîÙ¼©ýùÉ Û░òýá£Ùí£ Ýò¡ý▓┤ ý£áýáäý×ÉÙÑ╝ Týä©ÝżýùÉ ÙäúÛ│á Týä©ÝżÛ░Ç ÝÖ£ýä▒ÝÖöÙÉÿÙèö Ýøäýåì Û│╝ýáòýùÉ ÝòäýÜöÝò£ ýä©Ýż Ùé┤ ÙÂäý×ÉÙôñÙÅä Ýò¡ý▓┤ýÖÇ ýù░Û▓░Ýò┤ TCRýØä ÙîÇý▓┤ÝòÿÙèö ÔÇÿÛ▓░Ýò®ÙÉ£(chimeric) Ýò¡ýøÉ(antigen) ýêÿýÜ®ý▓┤(receptor)ÔÇÖ, ýªë, CARýØ┤ÙØ╝Ùèö Ù░®ýïØýØä ýô░Û▓î ÙÉ£Ùïñ. CARýØÇ 4Û░ÇýºÇ ýú╝ýÜö ÛÁ¼ýä▒ýÜöýåîÙí£ ýØ┤Ùú¿ýû┤ýá© ý×êÙèöÙì░, 1) ýä©ÝżýÖ© Ýæ£ýáü Ýò¡ýøÉ Û▓░Ýò® ÙÅäÙ®öýØ©(extracellular target antigen-binding domain), 2) Ý×îýºÇ ýÿüýù¡(hinge region), 3) ÙºëÝÜíÙï¿ ÙÅäÙ®öýØ©(transmembrane domain) Ù░Å 4) ÝòÿÙéÿ ýØ┤ýâüýØÿ ýä©Ýż Ùé┤ ýïáÝÿ©ýáäÙï¼ ÙÅäÙ®öýØ©(one or more intracellular signaling domains)ýØ┤ ÛÀ©Û▓âýØ┤Ùïñ. 1ýä©ÙîÇ CARýØÿ Û▓¢ýÜ░ ýä©ÝżÙé┤ ýïáÝÿ©ýáäÙï¼ ÙÅäÙ®öýØ©ýùÉ co-stimulatory moleculeýØ┤ ýùåýû┤ Ùï¿ýê£Ý×ê ýØ╝ýï£ýáüýØ© Týä©Ýż ýªØýïØ Ù░Å ýá£Ýò£ÙÉ£ ýé¼ýØ┤Ýåáý╣┤ýØ© ÙÂäÙ╣äÙÑ╝ ý£áÙÅäÝòÿýù¼ ÛÀ© ÝÜ¿Û│╝Û░Ç Ù»©Ù»©ÝòÿýÿÇÙïñ. Ýÿäý×¼ ÙäÉÙª¼ ýé¼ýÜ® ýñæýØ© 2ýä©ÙîÇ CARýØÿ Û▓¢ýÜ░, CD28 ÙÿÉÙèö 4-1BBýÖÇ Û░ÖýØÇ co-stimulatory moleculeýØ┤ ýä©ÝżÙé┤ ýïáÝÿ©ýáäÙï¼ ÙÅäÙ®öýØ©ýùÉ ÝåÁÝò®ÙÉÿýû┤ ýâØý▓┤ Ùé┤ýùÉýä£ CAR-T ýä©ÝżýØÿ ýâØýí┤Û│╝ Û©░ÙèÑýØä ý┤ëýºäÝòÿýù¼ ÝÜ¿Û│╝Û░Ç ÛÀ╣ÙîÇÝÖöÙÉÿýùêÙïñ[9-11]. CAR-T ýä©Ýż ý╣ÿÙúîýᣠÝè╣ýä▒ýâü ýòöýä©Ýż Ýæ£Ù®┤ýùÉ Ù¬àÝÖòÝò£ Ýæ£ýáü Ýò¡ýøÉýØ┤ ý×êýû┤ýò╝ Ýò┤ýä£, Ýÿäý×¼ ýè╣ýØ© Ù░øýØÇ ý╣ÿÙúîýá£ÙôñýØÇ Býä©ÝżýØÿ CD19 [12]ýÖÇ Býä©Ýż ýä▒ýêÖ Ýò¡ýøÉ(B-cell maturation antigen, BCMA) [13]ýØä Ýæ£ýáüý£╝Ùí£ Ýò£Ùïñ.
Ù│© Ùíá
CAR-T ýä©Ýż ý╣ÿÙúîýØÿ ýïñýá£
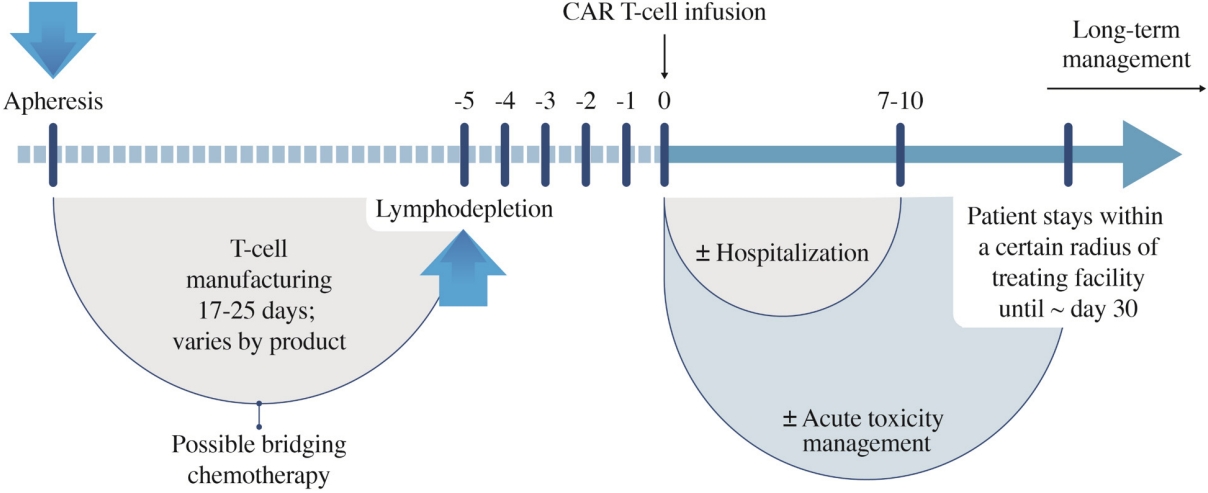
ýò×ýùÉýä£ ýû©Û©ëÝòÿýÿÇÙô»ýØ┤ CAR-T ýä©ÝżÙÑ╝ ý£áýáäÛ│ÁÝòÖýáüý£╝Ùí£ ýí░ý×æÝòÿÛ©░ ý£äÝò┤ Ù¿╝ýáÇ ýòöÝÖÿý×ÉýùÉýä£ Týä©ÝżÙÑ╝ ý▒äýºæÝò£Ùïñ(Fig. 1). ýØ┤ Týä©ÝżýùÉ Ù░öýØ┤Ùƒ¼ýèñÙÑ╝ ýØ┤ýÜ®Ýò£ ÝÿòýºêÙÅäý×à Û©░Ù▓òýØä ÝåÁÝò┤ ýòöýä©ÝżýùÉÙºî Ù░ÿýØæÝòÿÙèö Ýè╣ýØ┤ýáüýØ© ýêÿýÜ®ý▓┤ÙÑ╝ ÝÖÿý×ÉýØÿ Týä©ÝżýùÉ Ù░£Ýÿäýï£ÝéñÙÅäÙíØ ÝòÿÙèö ýâêÙí£ýÜ┤ ý£áýáä ýáòÙ│┤ÙÑ╝ ýú╝ý×àÝòÿÛ│á, ýØ┤ Týä©ÝżÙôñýØä Ù░░ýûæÝòÿýù¼ ÙîÇÙƒëý£╝Ùí£ ýªØýïØýï£Ýé¿Ùïñ. ýØ┤ Û│╝ýáòýØÇ ÙîÇÙ×Á 1Ùï¼ ýáòÙÅä ýåîýÜöÙÉÿÙèöÙì░, ýØ┤ Û©░Û░ä ÙÅÖýòê ÝÖÿý×ÉÙèö ÝòäýÜöýùÉ Ùö░ÙØ╝ Û░ÇÛÁÉ ý╣ÿÙúî(bridging therapy)ÙÑ╝ Ù░øÛ©░ÙÅä Ýò£Ùïñ. CAR-T ýä©Ýż ý╣ÿÙúîýá£Û░Ç ýÖäýä▒ýØ┤ ÙÉÿÙ®┤ ýáäý▓ÿý╣ÿ ýÜöÙ▓ò Ýøä ýä©Ýż ýú╝ý×àýØä ÝòÿÛ▓î ÙÉ£Ùïñ. ýØ┤Ùí£ýì¿ ýáòýâü ýä©Ýż ýåÉýâüýØÇ ýÁ£ýåîÝÖö ÝòÿÙ®┤ýä£ CARýØä Û░Çýºä Týä©ÝżÛ░Ç ÝÜ¿Û│╝ýáüý£╝Ùí£ ýòö ýä©ÝżÙÑ╝ ýé¼Ù®©ÝòÿÙÅäÙíØ Ýò£Ùïñ. Týä©ÝżýùÉ ÙºîÙôñýû┤ýºä Ùï¿Ù░▒ýºêýØ© CARýØÇ ýä©Ýż ýÖ©ÙÂÇýùÉýä£ ýòöýä©ÝżÙÑ╝ ýØ©ýïØÝòÿÙèö ýù¡ÝòáýØä ÝòÿÛ│á ýä©Ýż Ùé┤ÙÂÇýùÉýä£Ùèö Týä©ÝżÙÑ╝ ÝÖ£ýä▒ÝÖöÝòÿÙèö ýïáÝÿ©ÙÑ╝ ýáäÙï¼Ýòÿýù¼ ýòöýä©ÝżÙÑ╝ Û│ÁÛ▓®ÝòÿÙèö ýù¡ÝòáýØä Ýò£Ùïñ.
Ùª╝ÝöäýóàýùÉýä£ CAR-T ýä©Ýż ý╣ÿÙúîýá£
Ýÿäý×¼ USFDA ýè╣ýØ©ýØä Ù░øýØÇ CAR-T ýä©Ýż ý╣ÿÙúîýá£ÙÑ╝ ýé¼ýÜ®Ýòá ýêÿ ý×êÙèö Ùª╝ÝöäýóàýØÿ ýóàÙÑÿÙèö Û┤æÙ▓öý£äÝü░Býä©Ýż٪╝Ýöäýóà(diffuse large B cell lymphoma, DLBCL)Û│╝ ýÖ©Ýê¼ýä©Ýż٪╝Ýöäýóà(mantle cell lymphoma, MCL)ýØ┤ ý×êÙïñ. ýØ┤ ýñæýùÉýä£ÙÅä Ýè╣Ý×ê DLBCLýØÿ Û▓¢ýÜ░, ýÁ£ÛÀ╝ ý╣ÿÙúîýùÉ ý×êýû┤ Û░Çý×Ñ Ù╣áÙÑ┤Û│á ÙïñýûæÝò£ Ù│ÇÝÖöÛ░Ç ý×êýùêÙìÿ Ýÿêýòíýòöý£╝Ùí£, 2021ÙàäýØä Û©░ýáÉý£╝Ùí£ ýÜ░Ùª¼ÙéÿÙØ╝ýùÉýä£ÙÅä tisagenlecleucel ý╣ÿÙúîÛ░Ç Û░ÇÙèÑÝò┤ýíîÙïñ.
Axicabtagene ciloleucelý£╝Ùí£ ý×¼Ù░£ÙÂêýØæýä▒ DLBCLýùÉýä£ ýï£ÝûëÝò£ ZUMA-1 [2,14] ý×äýâüýï£ÝùÿýùÉýä£ ýÖäýáäÛ┤ÇÝò┤ý£¿ Ù░Å 12Û░£ýøö Ù¼┤ýºäÝûë ýâØýí┤ý£¿ýØÇ Û░üÛ░ü 58% Ù░Å 44%ýÿÇý£╝Ù®░, tisagenlecleucelÙí£ ý╣ÿÙúîÝò£ DLBCLýùÉýä£ ýñæýÂöýáüýØ© JULIET [5] ý×äýâüýï£ÝùÿýØÿ ýÖäýáäÛ┤ÇÝò┤ý£¿ýØÇ ýò¢ 40%ýÿÇÙïñ. ýØ┤Ùƒ¼Ýò£ Û▓░Û│╝Ùèö Ýæ£ 2ýùÉ ýÜöýò¢ÙÉÿýû┤ ý×êÙïñ.
TisagenlecleucelýØÿ Û▓¢ýÜ░ Ýÿäýí┤ÝòÿÙèö Û░Çý×Ñ ÝÜ¿Û│╝ýáüýØ© ý×¼Ù░£ÙÂêýØæýä▒ DLBCLýØÿ ý╣ÿÙúîÙ▓òýØ┤Ùïñ. ÙïñÙºî, 2ý░¿ýÜöÙ▓òý£╝Ùí£ ýé¼ýÜ®ÝòÿÛ©░ ý£äÝò£ 3ýâü ý×äýâüýï£ÝùÿýùÉýä£ ýÜ░ýøöÝòÿýºÇ Ù¬╗Ýò£ Û▓░Û│╝ÙÑ╝ Ù│┤ýù¼ýú╝ýû┤[15], axicabtagene ciloleucel, lisocabtagene maraleucel Ùô▒ Û▓¢ýƒü CAR-T ýá£ÝÆêÛ│╝ýØÿ Ù╣äÛÁÉýÜ░ý£äÙÑ╝ ýáÉÝòá ýêÿ ý×êýØäýºÇýùÉ ÙîÇÝò£ ýÜ░ÙáñÙÑ╝ ý×ÉýòäÙé┤Û│á ý×êÙïñ. Axicabtagene ciloleucelÛ│╝ lisocabtagene maraleucelýØÿ Û▓¢ýÜ░ 2ý░¿ýÜöÙ▓òý£╝Ùí£ ýé¼ýÜ®ÝòÿÛ©░ ý£äÝò£ ý×äýâüýï£ÝùÿýùÉýä£ tisagenlecleucelýÖÇ ÙïñÙÑ┤Û▓î[16] Û©░ýí┤ ý╣ÿÙúîÙ▓ò ÙîÇÙ╣ä ýÜ░ýøöÝò£ Û▓░Û│╝ÙÑ╝ Ù│┤ýù¼ýú╝ýû┤[14,16,17], tisagenlecleucelýùÉ Ù╣äÝòÿýù¼ ÝøäÙ░£ýú╝ý×Éý×äýùÉÙÅä ÙÂêÛÁ¼ÝòÿÛ│á ý×¼Ù░£ÙÂêýØæýä▒ DLBCLýØÿ ýâêÙí£ýÜ┤ ý╣ÿÙúîýá£Ùí£ýä£ýØÿ ýä▒Û│ÁýáüýØ© Ù░£ÝîÉýØä ÙºêÙá¿ÝòÿýÿÇÙïñ.
Axicabtagene ciloleucel [2,14,16]ýØÿ Û▓¢ýÜ░ tisagenlecleucelÛ│╝ ÙïñÙÑ┤Û▓î CD28 co-stimulationýØä ýé¼ýÜ®ÝòÿÙèö Û▓âýØ┤ Û░Çý×Ñ Ýü░ Ýè╣ýºòýØ┤Ùïñ. ZUMA-1 trialýØä ÝåÁÝò┤ ÛÀ© ÝÜ¿ÙèÑýØä ý×àýªØÝòÿýÿÇý£╝Ù®░, 3ýâüýØ© ZUMA-7 [17] Û▓░Û│╝ýùÉ ÛÀ╝Û▒░Ýòÿýù¼ 2022Ùàä 4ýøöÙÂÇÝä░ 1ý░¿ ý╣ÿÙúî Ýøä 12Û░£ýøö ýòêýùÉ ý×¼Ù░£ÝòÿýÿÇÛ▒░Ùéÿ 1ý░¿ ý╣ÿÙúîýùÉ ÙÂêýØæÝòÿÙèö ÝÖÿý×ÉÙôñýØä ÙîÇýâüý£╝Ùí£ ýé¼ýÜ®ýùÉ ÙîÇÝò┤ USFDA ýè╣ýØ©ýØä ýÀ¿ÙôØÝòÿýÿÇÙïñ.
Lisocabtagene maraleucel [5,18]ýØÇ tisagenlecleucelýØÿ ýá£ýí░Ù░®ýïØýØä Ù│ÇÝÿòÝòÿýù¼ CAR-T ýä©ÝżýØÿ ÝÜ¿ÙèÑýØä ýªØÛ░òÝòÿÛ│á ÙÂÇý×æýÜ®ýØä Û▓¢Û░ÉÝòÿÛ©░ ý£äÝò£ ýáäÙ×ÁýØä ýé¼ýÜ®ÝòÿýÿÇÙïñ. TRASCEND trialýØä ÝåÁÝòÿýù¼ ý×¼Ù░£ÙÂêýØæýä▒ DLBCLýùÉýä£ ÛÀ© ÝÜ¿ÙèÑýØä ý×àýªØÝòÿýÿÇý£╝Ù®░, 3ýâü TRANSFORM trial Û▓░Û│╝ýùÉ ÛÀ╝Û▒░Ýòÿýù¼ 2022Ùàä 6ýøöÙÂÇÙí£ USFDAýùÉýä£ 1ý░¿ ý╣ÿÙúî ýïñÝî¿ ýï£ ýé¼ýÜ®ýØä ýè╣ýØ©ÝòÿýÿÇÙïñ.
ÙïñÙ░£Û│¿ýêÿýóàýùÉýä£ CAR-T ýä©Ýż ý╣ÿÙúîýá£
ÙïñÙ░£Û│¿ýêÿýóàýùÉ ÙîÇÝò£ CAR-T ýä©Ýż ý╣ÿÙúîýᣠýù░ÛÁ¼Ùèö Ùª╝Ýöäýóà Ù░Å ALLýùÉ Ù╣äÝòÿÙ®┤ ýòäýºü ý┤êÛ©░ Ùï¿Û│äýØ┤Ùïñ. ýò×ýä£ýä£ÙÅä ýû©Û©ëÙÉÿýùêÙô»ýØ┤ Û░Çý×Ñ ÙäÉÙª¼ ýù░ÛÁ¼ÙÉ£ Û│¿ýêÿýóà CAR Ýæ£ýáüýØÇ BCMAÙí£ ýØ┤Ùèö ýóàýûæ Û┤┤ýé¼ ýØ©ý×É ýêÿýÜ®ý▓┤ ýèêÝì╝Ýî¿Ù░ÇÙª¼ ÛÁ¼ýä▒ýøÉ 17 (tumor necrosis factor receptor super family member 17, TNFRSF17)ýØ┤Ùïñ. BCMAÙèö Ýÿòýºê ýä©ÝżýùÉýä£Ùèö ýÜ░ýäáýáüý£╝Ùí£ Ù░£ÝÿäÙÉÿýºÇÙºî ýí░Ýÿê ýñäÛ©░ ýä©ÝżýùÉýä£Ùèö Ù░£ÝÿäÙÉÿýºÇ ýòèÛ©░ ÙòîÙ¼©ýùÉ ýØ┤ýâüýáüýØ© Ýæ£ýáü Ýò¡ýøÉýØ┤ÙØ╝ Ýòá ýêÿ ý×êý£╝Ù®░, Ùª¼Û░äÙô£ýØ© B-ýä©Ýż ÝÖ£ýä▒ÝÖö ýØ©ý×É(B-cell activating factor, BAFF) Ù░Å ýªØýïØ ý£áÙÅä Ùª¼Û░äÙô£(a proliferation-inducing ligand, APRIL)ýØÿ BCMAýùÉ ÙîÇÝò£ Û▓░Ýò® Ù░Å ý×ÉÛÀ╣ýØÇ Û│¿ýêÿýùÉýä£ Ýÿòýºê ýä©ÝżýØÿ ýä▒ý×Ñ Ù░Å ýªØýïØýØä ý┤ëýºäÝò£Ùïñ[19-21].
BCMA CAR-T ýä©Ýż ý╣ÿÙúîýá£ýØÿ ýäáÙæÉýú╝ý×ÉÙèö idecabtagene vicleucel [7]Ùí£, SFDAýùÉýä£ breakthrough-therapy designation awardÙÑ╝ Ù░øý£╝Ù®░ ÙïñÙ░£Û│¿ýêÿýóàýùÉýä£ÙÅä CARýØÿ ýï£ÙîÇÙÑ╝ ýù┤ýùêÙïñ. ÛÀ© Ýøä Ýò¡ýøÉ Û▓░Ýò® ý╣£ÝÖöÙÅäÙÑ╝ ÝûÑýâüýï£ÝéñÛ©░ ý£äÝò┤ 2Û░£ýØÿ BCMA Ýæ£ýáüÝÖö ÙÅäÙ®öýØ©ýØä ÝżÝò¿ÝòÿÙèö ýØ┤ýñæ epitope CAR-T ýä©Ýż ýá£ÝÆêýØ© JNJ-4528ÙÅä CARTITUDE-1 [22] ý×äýâüýï£ÝùÿýùÉýä£ ýØ©ýâüýáüýØ© 94.8%ýØÿ overall response rateÙÑ╝ Ù│┤ýù¼ýú╝ýùêÙïñ. ýØ┤ ýù░ÛÁ¼Ùèö CAR-T ýá£ÝÆêýØÿ Ùï¿ýØ╝ ýáÇýܮكë ýú╝ý×àýØ┤ ýí░Û©░ýùÉ Û╣èÛ│á ýºÇýåìýáüýØ© Ù░ÿýØæýØä ý£áÙÅäÝòÿÛ©░ýùÉ ý®ÙÂäÝòÿÙïñÙèö Û░òÙáÑÝò£ ýªØÛ▒░ÙÑ╝ ýá£Û│ÁÝòÿýÿÇÙïñ. ÙïñÙÑ© ýú╝Ù¬®ÝòáÙºîÝò£ BCMA CAR-T ýá£ÝÆêýØÇ ýØ┤ýïØÝÄ©ÙîÇýêÖýú╝Ù│æýØä ýñäýØ┤Û│á Týä©ÝżýØÿ ýºÇýåìýä▒ýØä ýù░ý×ÑÝòÿÙÅäÙíØ ýäñÛ│äÙÉ£ ýØ©Û░ä ý£áÙ×ÿ Ù░Å ýÖäýáä ýØ©Û░äÝÖö CAR (JCARH125) [22,23]ýØ┤Ùïñ. JCARH125ýØÿ ÝÜ¿ÙèÑýØÇ CD3+ ýê£ÙÅäÛ░Ç ÙåÆÛ│á ý┤êÛ©░ Û©░ýûÁ Ýæ£ÝÿäÝÿò Ù░Å ÙïñÛ┤ÇýÜ®ýä▒ýØ┤ ÝÆìÙÂÇÝò£ Týä©Ýż ýá£ÝÆêÛ│╝ Û┤ÇÙá¿ýØ┤ ý×êÙèö Û▓âý£╝Ùí£ Ù│┤Û│áÙÉÿýùêÙïñ(Table 3).
CAR-T ýä©Ýż ý╣ÿÙúîýᣠÙÂÇý×æýÜ®
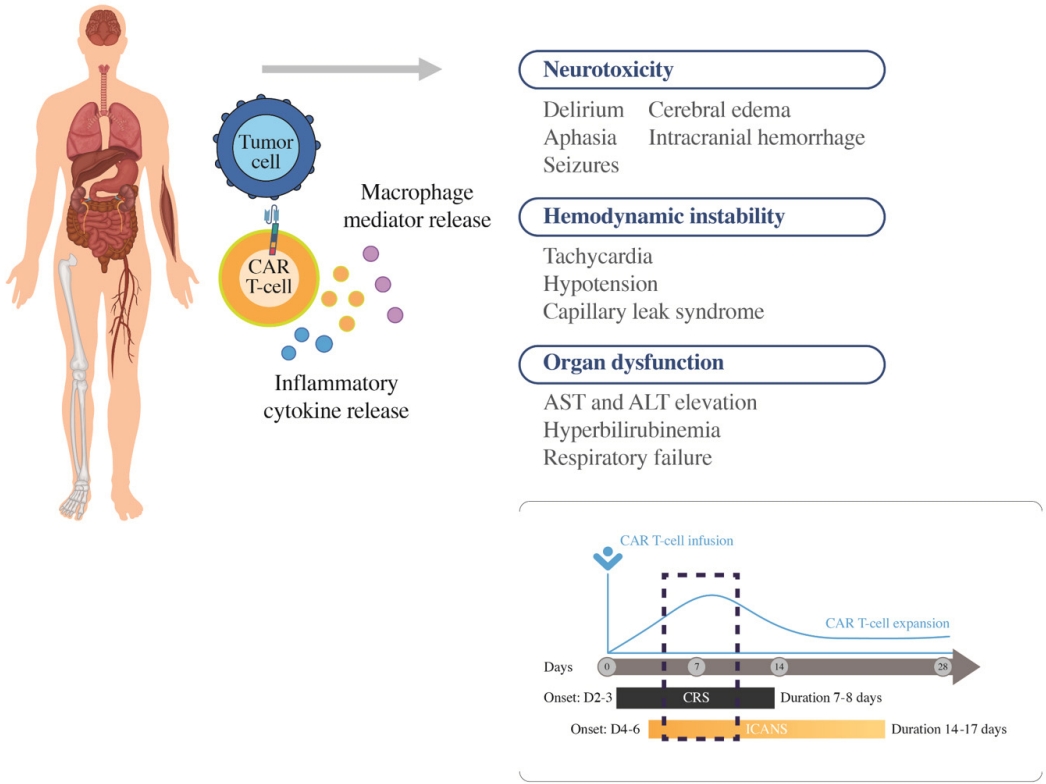
Û░Çý×Ñ ýú╝Ù¬®Ýò┤ýò╝ ÝòÿÙèö ÙÂÇý×æýÜ®ý£╝Ùí£Ùèö ýé¼ýØ┤Ýåáý╣┤ýØ© ÙÂäÙ╣ä ýªØÝøäÛÁ░(cytokine release syndrome, CRS)Û│╝ ýïáÛ▓¢ÙÅàýä▒ ýªØÝøäÛÁ░(immune effector cell associated neurotoxicity syndrome, ICANS)ýØ┤ ý×êÙïñ[24]. ÛÀ© Ù╣êÙÅäÙèö Û░ü CAR-T ýä©Ýż ý╣ÿÙúîýá£ýØÿ ýܮكë, CARýØÿ ÛÁ¼ýí░(e.g CD28 costimulatory molecule ýé¼ýÜ® ýï£ ÙåÆýØÇ Ù╣êÙÅäÙí£ Ù░£ýâØ), Ù│æýØÿ ýóàÙÑÿ Ù░Å ýáòÙÅä, ÝÖÿý×ÉýØÿ ýâüÝâ£ýùÉ Ùö░ÙØ╝ Ùï¼ÙØ╝ýºê ýêÿ ý×êÙïñ(Fig. 3).
CRSýØÿ Û▓¢ýÜ░ CAR-TýØÿ ÝÖ£ýä▒ÝÖö Ù░Å ýªØýïØÛ│╝ Ýò¿Û╗ÿ ýù╝ýªØýä▒ ýé¼ýØ┤Ýåáý╣┤ýØ©(IL-1╬▓, IL-6, IL-10, chemokines [CXCL8, CCL2], interferon-╬│, granulocyte-macrophage colony-stimulating factor and tumor necrosis factor)ýØÿ ÙÂäÙ╣ä ýªØÛ░ÇÙí£ ýØ©Ýò┤ ýâØÛ©░Ùèö Û▓âý£╝Ùí£, ÙîÇÙÂÇÙÂä CAR-T ýä©Ýż ý╣ÿÙúîýᣠýú╝ý×à Ýøä 2-3ýØ╝ Ùé┤ Ù░£ýâØÝòÿýù¼ 7-8ýØ╝ ýáòÙÅä ýºÇýåìÙÉÿÙèö Û▓âý£╝Ùí£ ýòîÙáñýá© ý×êÙïñ[25]. ý╣ÿÙúîÙÑ╝ ýÜöÝòÿÙèö CRSýØÿ Ù╣êÙÅäÙèö 7-47% ýáòÙÅäÙí£ Ù│┤Û│áÙÉÿýû┤ ý×êÙïñ. CRSýØÿ Ù│æÝâ£ýâØÙª¼Ùèö Ùïñýä» Û░ÇýºÇ ýú╝ýÜö Ùï¿Û│äÙí£ ÙéÿÙêî ýêÿ ý×êÙïñ. CRSýÖÇ Û┤ÇÙá¿ÙÉ£ ýªØýâü Ù░Å ýºòÝøäýùÉÙèö Û│áýù┤, ýÿñÝò£, Û▓¢ýºü, ÙÅÖýä▒ Ù╣êÙºÑ, ÛÀ╝ý£íÝåÁ Ù░Å Ýö╝Ùí£Û░Ç ÙîÇÝæ£ýáüýØ┤Ùïñ. ýáÇÝÿêýòò, ýáÇýé░ýåîýªØ, ÙÂÇýáòÙºÑ, ýï¼ý×Ñ Ù░òý£ÙÑá ýáÇÝòÿ Ù░Å Û©░ÝâÇ ÙºÉÙï¿ Û©░Û┤Ç Û©░ÙèÑ ý×ÑýòáýÖÇ Û░ÖýØÇ Ùìö ýï¼Û░üÝò£ ÙÅàýä▒ÙÅä Ù░£ýâØÝòá ýêÿ ý×êÙïñ. ÙÿÉÝò£ CRSýÖÇ Û┤ÇÙá¿ÙÉ£ ý×ÑÛ©░ ÙÅàýä▒ýùÉÙèö Û░Çýù¡ýáü ýïáÙÂÇýáä, Û░ä ÝÜ¿ýåî ýâüýè╣, ýáäÝò┤ýºê Û│áÛ░ê, ÝÿêÛÁ¼Û░ÉýåîýªØ Ù░Å ýØæÛ│áÙ│æýªØ Ùô▒ýØ┤ ý×êÙïñ. CRS Grading systemýØÇ ýù¼Ùƒ¼ Û░ÇýºÇÛ░Ç ý×êý£╝Ùéÿ Û░Çý×Ñ ÙäÉÙª¼ ýé¼ýÜ®ÙÉÿÙèö Û▓âýØÇ Lee Ùô▒[24]ýØ┤ Ù│┤Û│áÝò£ American Society for Transplantation and Cellular Therapy (ASTCT) gradingý£╝Ùí£ Ýæ£ 4ýùÉ ýáòÙª¼ÙÉÿýû┤ ý×êÙïñ.
Ù░ÿÙ®┤ ICANSÙÑ╝ ÝżÝò¿Ýò£ ýïáÛ▓¢ÙÅàýä▒ýØÿ Û▓¢ýÜ░, ÝÿêýòíÙçîý×ÑÙ▓¢ýØä ÝåÁÛ│╝Ýò£ Týä©Ýż, Ùï¿ÝòÁÛÁ¼ Ùô▒ýùÉ ýØÿÝòÿýù¼ ÙÂäÙ╣äÙÉ£ ýé¼ýØ┤Ýåáý╣┤ýØ©ýØ┤ Û┤Çýù¼ÝòÿÙèö Û▓âý£╝Ùí£ ýòîÙáñýá© ý×êý£╝Ù®░, CRSÙ│┤Ùïñ ýí░Û©ê ÙèªýØÇ ýï£Û©░ýØ© CAR-T ýä©Ýż ý╣ÿÙúîýᣠýú╝ý×à Ýøä 4-6ýØ╝ýùÉ Ù░£ýâØÝòÿýù¼ 14-17ýØ╝ ýáòÙÅä ýºÇýåìÙÉÿÙèö Û▓âý£╝Ùí£ ýòîÙáñýá© ý×êÙïñ. ICANSýØÿ ý┤êÛ©░ ýªØýâüýùÉÙèö Ýæ£Ýÿäýä▒ ýïñýû┤ýªØ, Ùû¿Ùª╝, Ùé£ýï£ Ù░Å Ýÿ╝ýêÿÛ░Ç ý×êÙïñ. ýØ┤Ùƒ¼Ýò£ ýªØýâüýØÇ ýáäý▓┤ ýïñýû┤ýªØ, Ù░£ý×æ, ÙæöÛ░É, Ýÿ╝Ù»© Ù░Å Ýÿ╝ýêÿ ýâüÝâ£Ùí£ ýºäÝûëÙÉá ýêÿ ý×êÙïñ.
Ýæ£ 5ýùÉ CRSýÖÇ ICANSýØÿ ý╣ÿÙúîÛ░Ç ýáòÙª¼ÙÉÿýû┤ ý×êÙïñ. Ùé«ýØÇ Ùô▒Û©ëýØÿ CRSÙèö Û░Éýù╝Û│╝ Û░ÖýØÇ Ù░£ýù┤ýØÿ ÙïñÙÑ© ÙÅÖÙ░ÿ ýøÉýØ©ýØ┤ ýùåÙèöýºÇ ÝÖòýØ©ÝòÿÙ®┤ýä£ Ýò┤ýù┤ýá£ÙÑ╝ ÝåÁÝò£ ýºÇýºÇýÜöÙ▓òý£╝Ùí£ Û┤ÇÙª¼Ýò£Ùïñ. ýñæÙô▒ÙÅäýùÉýä£ ýñæýªØ CRSÙèö IL-6R ý░¿Ùï¿ Ýò¡ý▓┤ýØ© ÝåáýïñÙª¼ýú╝ÙºÖ(tocilizumab)Û│╝ Ýò¿Û╗ÿ ÝòäýÜö ýï£ ý¢öÙÑ┤Ýï░ý¢öýèñÝàîÙí£ýØ┤Ùô£ÙÑ╝ Ýò¿Û╗ÿ ýé¼ýÜ®Ýò£Ùïñ. Ùé«ýØÇ Ùô▒Û©ëýØÿ ICANSÙèö ÙÿÉÝò£ ýØ╝Ù░ÿýáüý£╝Ùí£ ýºäÙï¿ ýáòÙ░Ç Û▓Çýé¼ýÖÇ ýºÇýºÇýÜöÙ▓òý£╝Ùí£ Û┤ÇÙª¼ÙÉÿÙèö Ù░ÿÙ®┤, ýñæýªØ ICANSÙèö ÙîÇÛ░£ ÙîÇÙÂÇÙÂäýØÿ Û▓¢ýÜ░, ý¢öÙÑ┤Ýï░ý¢öýèñÝàîÙí£ýØ┤Ùô£ ý╣ÿÙúîÙÑ╝ ÝòÿÛ▓î ÙÉ£Ùïñ. ÝåáýïñÙª¼ýú╝ÙºÖýØÿ ýé¼ýÜ®ýØÇ ýï¼Û░üÝò£ CRSýØÿ Ù░£Ù│æÙÑáýØä ÝÿäýáÇÝ×ê Û░Éýåîýï£ý╝░ÙèöÙì░, IL-6Û░Ç downstream inflammatory cascadeýØÿ ÝòÁýï¼ ÙºñÛ░£ý▓┤ýØ┤Ù®░, CRS ý┤êÛ©░ýùÉ ýÁ£Û│áýí░ýùÉ ÙïñÙïñÙÑ┤Û©░ ÙòîÙ¼©ýØ┤Ùïñ. ÙïñÙºî ý¢öÙÑ┤Ýï░ý¢öýèñÝàîÙí£ýØ┤Ùô£Ùèö CAR-T ýä©Ýż Ù░Å Û©░ÝâÇ Ù░®Û┤Çý×É Ù®┤ýù¡ ýä©Ýż, Ýè╣Ý×ê Û│¿ýêÿ ýä©ÝżýØÿ ýªØýïØ Ù░Å ýé¼ýØ┤Ýåáý╣┤ýØ© ÙÂäÙ╣ä ýûÁýá£ÙÑ╝ ÝżÝò¿Ýòÿýù¼ ýáäý▓┤ýáüýØ© Ù®┤ýù¡ ýûÁýá£ÙÑ╝ ý£áÙÅäÝòá ýêÿ ý×êÛ©░ ÙòîÙ¼©ýùÉ ýï¼Û░üÝò£ ýâüÝÖ®ýùÉýä£Ùºî Ýò¿Û╗ÿ Û│áÙáñÙÑ╝ Ýò┤ýò╝ Ýò£Ùïñ.
ÝåáýïñÙª¼ýú╝ÙºÖýØÿ Û▓¢ýÜ░, CRSýØÿ Û┤ÇÙª¼ýùÉ ÙºñýÜ░ ÝÜ¿Û│╝ýáüýØ┤ýºÇÙºî ICANSýØÿ Û▓¢ýÜ░ ÙîÇÙÂÇÙÂäýùÉýä£ÝÜ¿Û│╝Û░Ç ýùåÙïñ. ýØ┤Ùèö CRSýÖÇ ICANS ýé¼ýØ┤ýØÿ Ù│æÝâ£ýâØÙª¼ÝòÖýáü ý░¿ýØ┤ Ù░Å/ÙÿÉÙèö BBBÙÑ╝ ÝåÁÝò£ ÝåáýïñÙª¼ýú╝ÙºÖýØÿ Ù╣êýò¢Ýò£ ý╣¿Ýê¼ ÙòîÙ¼©ýØ┤ÙØ╝Û│á ýâØÛ░üÝò£Ùïñ. ýïñýá£Ùí£, ÝåáýïñÙª¼ýú╝ÙºÖýØÿ ýÿêÙ░®ýáü ýé¼ýÜ®ýØÇ ýï¼Û░üÝò£ CRSýØÿ Ù░£ýâØýØä Û░Éýåîýï£ý╝░ýºÇÙºî ÙÉÿÙáñ ýï¼Û░üÝò£ ICANSýØÿ Ù░£ýâØýØä ýªØÛ░Çýï£ý╝░ÙèöÙì░, ýØ┤Ùèö ýòäÙºêÙÅä ÝåáýïñÙª¼ýú╝ÙºÖ Ýê¼ýù¼ Ýøä Û┤Çý░░ÙÉÿÙèö Ýÿêý▓¡ IL-6 ýêÿý╣ÿýØÿ Û░ÉýåîÙí£ ýØ©Ýò┤ ýêÿýÜ®ý▓┤ ý░¿Ùï¿ýùÉ ýØÿÝò┤ ÙºÉý┤ê ýí░ýºüý£╝Ùí£ýØÿ ÝØíýêÿÙÑ╝ Ù░®ýºÇÝòÿýÿÇÛ©░ ÙòîÙ¼©ýØ┤Ùïñ. ýØ┤ýùÉ ICANS ý╣ÿÙúîýùÉ ÛÀ╝Û░äýØ┤ ÙÉÿÙèö Û▓âýØÇ ý¢öÙÑ┤Ýï░ý¢öýèñÝàîÙí£ýØ┤Ùô£ýØ┤Ùïñ. ÙîÇÙÂÇÙÂäýØÿ ýù░ÛÁ¼ýùÉ Ùö░ÙÑ┤Ù®┤ ÝåáýïñÙª¼ýú╝ÙºÖýØÿ ýé¼ýÜ®ýØÇ CAR-T ýä©ÝżýØÿ ÝÜ¿ÙèÑýùÉ ýÿüÝûÑýØä Ù»©ý╣ÿýºÇ ýòèÙèö Û▓âý£╝Ùí£ Ù│┤ýØ┤Ùéÿ, ý¢öÙÑ┤Ýï░ý¢öýèñÝàîÙí£ýØ┤Ùô£ýØÿ ýé¼ýÜ®ýØÇ ýí░Û©░ ýºäÝûë Ù░Å ýé¼ÙºØ ý£äÝùÿýØ┤ ýªØÛ░ÇÝòÿÙèö ÙÂêÙª¼Ýò£ ý×äýâü Û▓░Û│╝ÙÑ╝ Ù│┤ýØ© Ù░ö ý×êÛ©░ ÙòîÙ¼©ýùÉ CRS Ù░Å ICANSýØÿ Ù│æÝâ£ýâØÙª¼ÝòÖýáü Ù®öý╗ñÙïêýªÿýùÉ ÙîÇÝò£ Ùìö ÙéÿýØÇ ýØ┤Ýò┤ýÖÇ ýØ┤ÙôñýØÿ Û┤ÇÙª¼ÙÑ╝ ý£äÝò£ ýâêÙí£ýÜ┤ ýáäÙ×Á Û░£Ù░£ýØ┤ ÝòäýÜöÝòÿÙïñ[25].
CAR-T ýä©Ýż ý╣ÿÙúîýØÿ ý×ÑÛ©░ ÙÅàýä▒ý£╝Ùí£Ùèö Û░Éýù╝ ý£äÝùÿýØä ýªØÛ░Çýï£Ýé¼ ýêÿ ý×êÙèö ýáÇÛ░ÉÙºêÛ©ÇÙí£ÙÂêÙª░ÝÿêýªØ Ù░Å ÝÿêÛÁ¼Û░ÉýåîýªØýØä ý£áÙ░£ÝòÿÙèö Býä©Ýż Ù¼┤Ýÿòýä▒ýØ┤ ÝżÝò¿ÙÉ£Ùïñ. ýòàýä▒ Býä©ÝżýÖÇ ýáòýâü Býä©Ýż Ù¬¿ÙæÉ Ýæ£Ù®┤ýùÉýä£ CD19ÙÑ╝ Ù░£ÝÿäÝòÿýù¼ Ýò¡-CD19 CAR-T ýä©Ýż ýÜöÙ▓ò Ýøä "on-target, off-tumor" Býä©Ýż Ù¼┤Ýÿòýä▒ýØä ý£áÙ░£Ýòá ýêÿ ý×êÙïñ. Býä©Ýż Ù¼┤Ýÿòýä▒ýØÇ ý×áý×¼ýáüý£╝Ùí£ ýêÿÛ░£ýøöýùÉýä£ ýêÿÙàä ÙÅÖýòê ýºÇýåìÙÉá ýêÿ ý×êý£╝Ù®░ Ù╣êÙ▓êÝò£ Û░Éýù╝ý£╝Ùí£ ýØ┤ýû┤ýºê ýêÿ ý×êÛ©░ ÙòîÙ¼©ýùÉ, ÝòäýÜö ýï£ Ù®┤ýù¡Û©ÇÙí£ÙÂêÙª░ ý╣ÿÙúîÛ░Ç ÝòäýÜöÝòÿÙïñ. ÙìöÙÂêýû┤ Ù®┤ýù¡ ÙºñÛ░£ Ù▓öÝÿêÛÁ¼Û░ÉýåîýªØýØä ý£áÙ░£Ýòá ýêÿ ý×êÛ©░ ÙòîÙ¼©ýùÉ ýÁ£ýåî 6Û░£ýøö ýØ┤ýâü ýÂöýáü Û┤Çý░░ýØä ÝòÿÙ®░ ýáüýáòÝò£ ýêÿÝÿê Ù░Å ýä▒ý×Ñ ýØ©ý×É ýºÇýøÉýØ┤ ÝòäýÜöÝòÿÙïñ[26-28].
Û▓░ Ùíá
CAR-T ýä©Ýż ý╣ÿÙúîýá£Û░Ç Ýè╣ýáò Ýÿêýòíýòö ý╣ÿÙúîýùÉ ÝÿüýïáýáüýØ© Ù│ÇÝÖöÙÑ╝ ýØ╝ý£╝Ýé¿ Û▓âýØÇ ÝïÇÙª╝ýØ┤ ýùåÙïñ. ÝòÿýºÇÙºî ýØ┤ Ù│Áý×íÝòÿÛ│á ýºäÝÖöÝòÿÙèö ÙÂäýò╝ýØÿ ýÜöÛÁ¼ ýé¼Ýò¡ýØä ý®ýí▒ÝòÿÛ©░ ý£äÝò┤ ýØ©ÙáÑýØä ÛÁÉý£íÝòÿÙèö Û▓âýØÇ ýû┤ÙáñýÜ┤ ýØ╝ýØ┤Ù®░ ýØ┤ýùÉ Ùº×ýÂöýû┤ ý╗ñÙª¼ÝüÿÙƒ╝ Û░£Ù░£ýØ┤ ÝòäýÜöÝòÿÙïñ. ÙÿÉÝò£ ÙºîÙºîý╣ÿ ýòèýØÇ ý╣ÿÙúî Ù╣äýÜ® Ùô▒ ÝÆÇýû┤ýò╝ ÝòÿÙèö Û│╝ýá£Û░Ç ý×êÙïñ. ÙïñÙºî ýù¼Ùƒ¼ ý×äýâüýï£ÝùÿÛ│╝ ýïñýᣠý×äýâü Ýÿäý×ÑýùÉýä£ Û▓¢ÝùÿýØ┤ ýÂòýáüÙÉ¿ýùÉ Ùö░ÙØ╝ Ùï¿ÝÜîýØÿ CAR-T ýï£ýêáÙí£ ýÖäý╣ÿ Û░ÇÙèÑýä▒ýØ┤ Û┤Çý░░ÙÉÿÛ│á ý×êýû┤, ý┤êÛ©░ýØÿ ÙåÆýØÇ Ù╣äýÜ®Û│╝ ÙºÄýØÇ ýØ©ýáü, Ù¼╝ýáü Ýê¼ý×ÉÛ░Ç ÝòäýÜöÝòÿÙïñÛ│á ýØ©ýáòÙÉá Û░ÇÙèÑýä▒ýØ┤ ÙåÆÙïñ.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






