


증 례
27세 남자가 1년 전부터 발생한 역류 증상, 가슴답답함 및 체중감소로 내원하였다. 6개월 전 개인의원에서 내시경 검사를 시행하여 역류성식도염 외 특이 소견이 없어 proton pump inhibitor (PPI)를 포함한 약물을 3개월간 복용하였으나 증상이 더욱 심해져 최근에는 물도 삼키기 힘들어졌다고 한다.
진단의 일차 단계
본원에서 시행한 내시경에서 위식도접합 부위에 미란 등은 관찰되지 않았고 위식도접합부(esopahgogastric junction, EGJ) 통과 시 약간의 저항감만 느껴졌다. PPI를 장기간 복용함에도 불구하고 증상이 오히려 악화되었으며, 최근에는 삼킴곤란 증상까지 발생하여 식도운동 질환이 의심되어 고해상도 식도내압 검사를 시행하였다. 고해상도 식도내압 검사상 하부식도 괄약근의 이완시 압력인 integrated relaxation pressure (IRP) 값이 24.7 mmHg로 상승되어 있었으며 식도연동운동은 소실되었고 panesophageal pressurization 소견을 보였다(Fig. 1).
최종 진단과 치료 경과
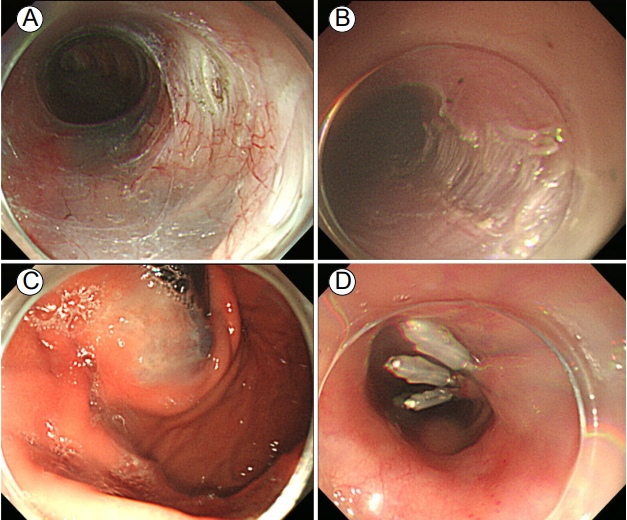
고해상도 식도내압 검사상 type II achalasia로 진단되었고 환자의 Eckardt 증상 점수는 11점이었다. 치료 계획으로 풍선확장술과 경구 내시경 근절개술(peroral endoscopic myotomy, POEM)을 고려하였으며 환자와 상의하여 경구 내시경 근절개술을 시행하기로 하였다. 경구 내시경 근절개술은 전신마취 하에 수술실에서 진행되었고 위식도접합부 하부 2 cm를 포함하여 총 14 cm의 길이로 근절개를 시행하였다(Fig. 2). 시술 후 환자의 Eckardt 증상 점수는 11점에서 1점으로 감소하였고 고해상도 식도내압 검사 소견도 IRP 값이 24.7 mmHg에서 7.4 mmHg로 감소하였다(Fig. 3). 시술 후 1년 경과 시까지 증상의 재발이 보이지 않고 잘 유지되고 있다.
고 찰
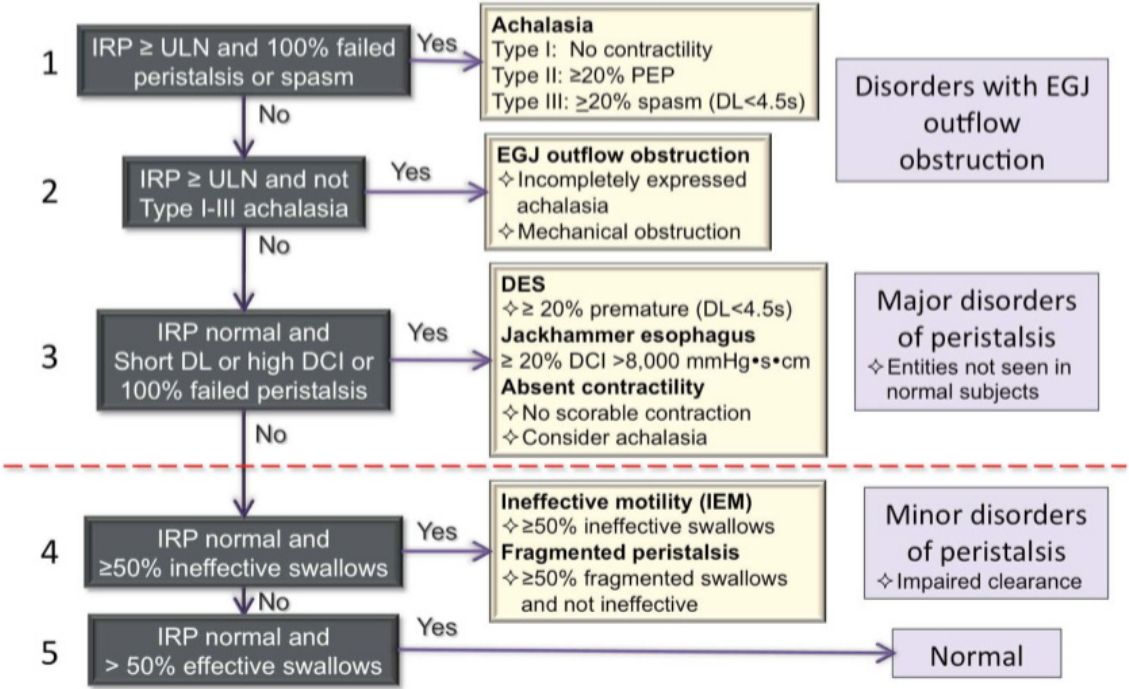
고해상도 식도내압 검사는 기존의 식도내압 검사에 비하여 압력 센서가 치밀하게 분포하여 식도운동 변화를 보다 세밀하게 측정할 수 있다. 이 기기의 도입으로 식도운동 질환의 진단에 있어 획기적인 발전이 이루어졌을 뿐 아니라 식도운동 질환의 정의와 분류마저 새로이 정립되었다. 고해상도 식도내압 검사 결과를 기반으로 식도운동 질환의 새로운 분류법이 만들어지게 되었는데 처음 버전은 2008년 샌디에고에서 열렸던 International HRM Working Group 회의를 통하여 제시되었다[1]. 이후 몇 번의 수정을 거쳐 2014년 Chicago에서 세계 각국의 소화기운동학회 관련 연구자들이 모여 회의한 결과 지금 현재 사용되고 있는 Chicago classification v3.0이 만들어지게 되었다[2]. 고해상도 식도내압 검사에서는 압력 수치 이외에 다양한 지표들이 측정 가능한데(Table 1) [2], 이러한 지표들은 크게 수축 강도, 수축 패턴, 삼킴 시 30 mmHg 등압 윤곽선 패턴에 따라 여러 가지의 비정상 운동 패턴으로 분류된다(Table 2) [2]. Chicago classification은 이러한 여러 가지 지표와 운동 패턴을 계층적으로 분석하여 다양한 형태의 식도운동 질환을 진단할 수 있도록 도와준다(Fig. 4) [3]. 아칼라지아의 경우 Chicago classification에 따라 1형, 2형, 3형으로 분류할 수 있으며 식도체부의 연동운동은 정상이지만 하부식도괄약근의 이완에 장애가 있는 위식도접합부 폐쇄(EGJ outflow obstruction, EGJOO)라는 새로운 카테고리의 질환도 진단할 수 있게 되었다. 업데이트된 Chicago classification을 적용할 경우 기존의 분류법에 비하여 진단이 불명확한 경우와 주요 운동 질환(major motor disorder)의 빈도가 줄어든 대신 위식도접합부 폐쇄나 사소한 운동 질환(minor motor disorder)의 빈도가 늘어난 것으로 보고되고 있다[3].


 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






