


서론
자가면역간염(autoimmune hepatitis, AIH)은 주로 중년의 여성에서 호발하는 원인 미상의 만성 간질환으로 임상적으로 혈청 아미노전이효소(AST와 ALT)의 상승, 고감마글로불린혈증과 함께 자가면역항체 출현이 관찰되며 조직학적으로는 계면간염(interface hepatitis)을 특징으로 하는 질환이다[1]. 특정한 유전적 감수성을 가진 사람에서 환경적인 요인으로 발생하며, 유발 원인으로는 바이러스 감염(A형 간염, 엡스타인바, 인간 헤르페스 6, 홍역 등), 약물, 약초 복용 등이 있다[2]. 대략 25%에서 급성 간염이나 만성 간질환의 급성 악화의 형태로 나타나며 1/3의 환자에서 진단 당시 간경변증을 보인다. 치료하지 않는 경우 비대상성 간경변증, 간부전 및 사망으로 이어질 수 있다[3]. 본고에서는 마이코플라즈마 감염 후 발생한 자가면역간염에 대한 증례를 통해 자가면역간염의 진단적 접근에 대해 정리해 보고자 한다.
본론
증례
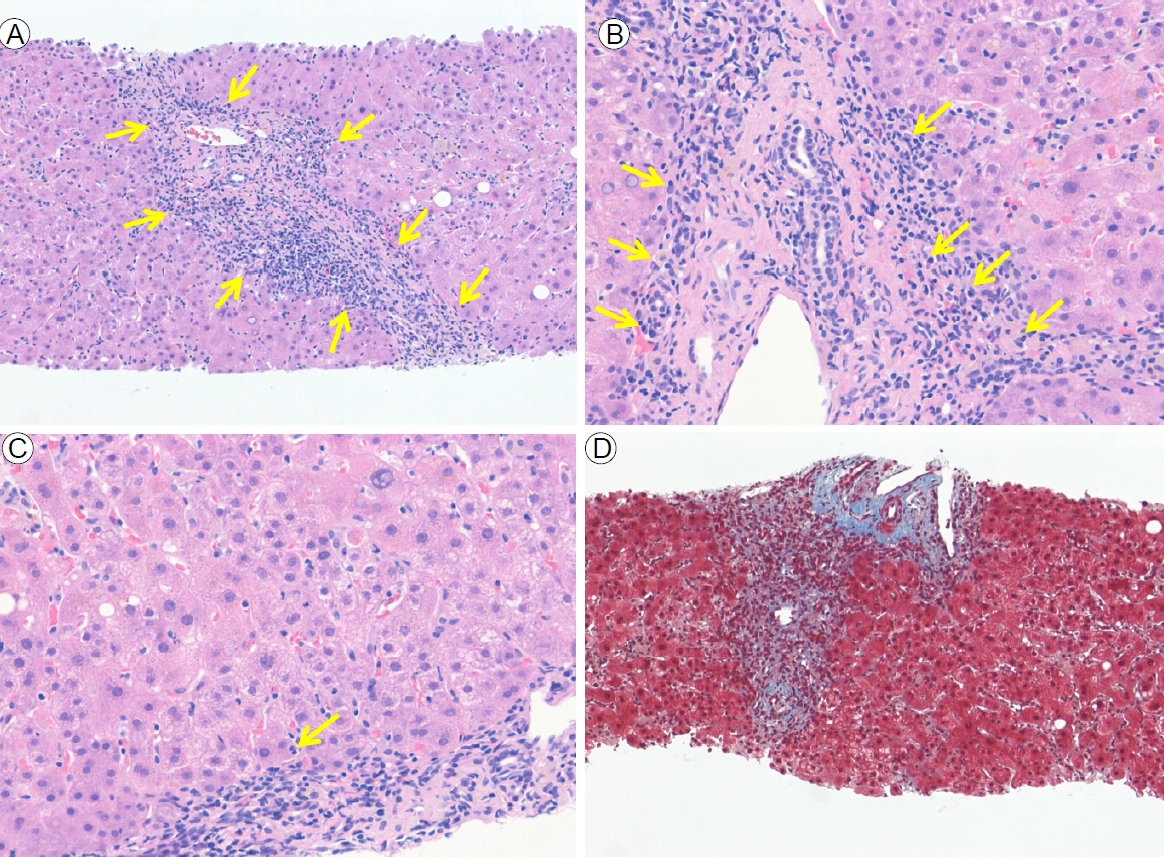
기저 질환으로 기관지확장증을 가진 58세 여자가 3주간 발열을 동반한 기침과 객혈 증상으로 호흡기내과에 입원하였다. 혈청 폐렴 마이코플라즈마 항체 양성으로 확인되어 마이코플라즈마 폐렴 진단으로 항생제(록시스로마이신 300 mg/day) 치료를 시작하였고, 이후 기침과 객혈 등의 증상은 호전되었다. 하지만 입원 3일째 혈액 검사에서 황달을 동반하지 않는 지속적인 혈청 아미노전이효소 증가(AST 418 IU/L, ALT 164 IU/L)를 보였고, 7일간 항생제를 복용 후 중단하였음에도 지속적인 혈청 아미노전이효소의 상승(AST 919 IU/L, ALT 987 IU/L)이 확인되었다. 복부 전산화단층촬영술에서는 간비대 이외의 특이 소견은 관찰되지 않았다. 환자는 정상 체중으로 음주력은 없었고 평소 복용 중인 약제도 없었다. 간염의 원인을 확인하기 위해 추가적인 혈액 검사를 시행하여 바이러스간염 등은 배제할 수 있었고, 항핵항체(antinuclear antibody, ANA) 1:80, 면역글로불린 G (immunoglobulin G, IgG) 2,376 mg/dL로 증가되어 자가면역간염의 진단을 위해 간 생검을 시행하였다. 조직 검사에서 중등도의 계면간염(interface hepatitis)과 형질세포 침투를 확인하였고(Fig. 1), 이를 반영한 개정된 International Autoimmune Hepatitis Group (IAIHG) 에 따른 자가면역간염 진단을 위한 점수는 16으로 명확한 자가면역간염에 합당하였다[4]. 치료로 경구 프레드니솔론 60 mg을 복용한 이후 혈청 아미노전이효소는 급격히 감소하였으며, 아자티오프린 추가 및 프레드니솔론 감량에도 혈청 아미노전이효소 및 IgG는 정상 범위까지 회복되었다.
자가면역간염의 병태생리 및 임상 소견
자가면역간염은 전 연령층과 모든 인종에서 발생할 수 있으며, 어른과 소아 모두 여성에서 호발(남여 비 약 1:3)하는 것으로 알려져 있다[5]. 추정 발병률은 지역과 발병 연령에 따라 다양하며, 유병률은 유럽 인구 100,000명당 11-25명이며 여성과 남성 모두에서 증가하고 있다[6]. 최근 연구에 따르면, 한국에서 자가면역간염은 중년(중위 연령 56세) 여성 (남녀 비 1:6.4)에서 호발하며, 유병률은 인구 100,000명당 4.82명이고 발생률은 인구 100,000명당 1.07로 확인되었다. 유럽이나 북미와 비교하여 적은 수로, 이는 환경적 및 유전적 차이로 인한 것으로 보인다[7].
자가면역간염은 유전적, 후성적, 면역학적, 환경적 요인의 상호 작용이 필요한 복합 유전 질환이다. 환경적 요인은 유전적 요인보다 면역 레퍼토리를 형성하는 데 중요한 역할을할 수 있으며, 특정한 환경적 요인(바이러스 감염이나 생체 이물에 대한 노출)은 유전적으로 자가면역간염에 취약한 사람에게서 자가 항원에 대한 자기 내성 상실을 유발할 수 있다[8].
자가면역간염은 무증상에서 급성/중증 또는 전격성 간염까지 임상적으로 다양하게 발현될 수 있다. 대부분의 자가면 역간염 환자는 피로, 권태감, 관절통 또는 무월경 등의 만성적인 비특이적 증상을 호소하며, 85%의 환자가 피로감을 주로 호소한다[9]. 진행성 만성 간질환의 징후(거미 모반, 비장 비대, 복수 등) 또는 간 외 자가면역 질환(백반증, 염증성 장질환)의 징후를 제외하고 신체적인 징후는 일반적으로 나타나지 않는다[10]. 또한 자가면역간염 환자의 25-34%는 무증상 환자이나 증상이 있는 환자와 유사한 조직학적 소견을 보이며, 2-120개월 이내에 증상이 발생하는 경우가 많으므로 증상의 부재를 이유로 치료를 시작하지 않아서는 안 된다[11-13].
자가면역간염의 진단 기준
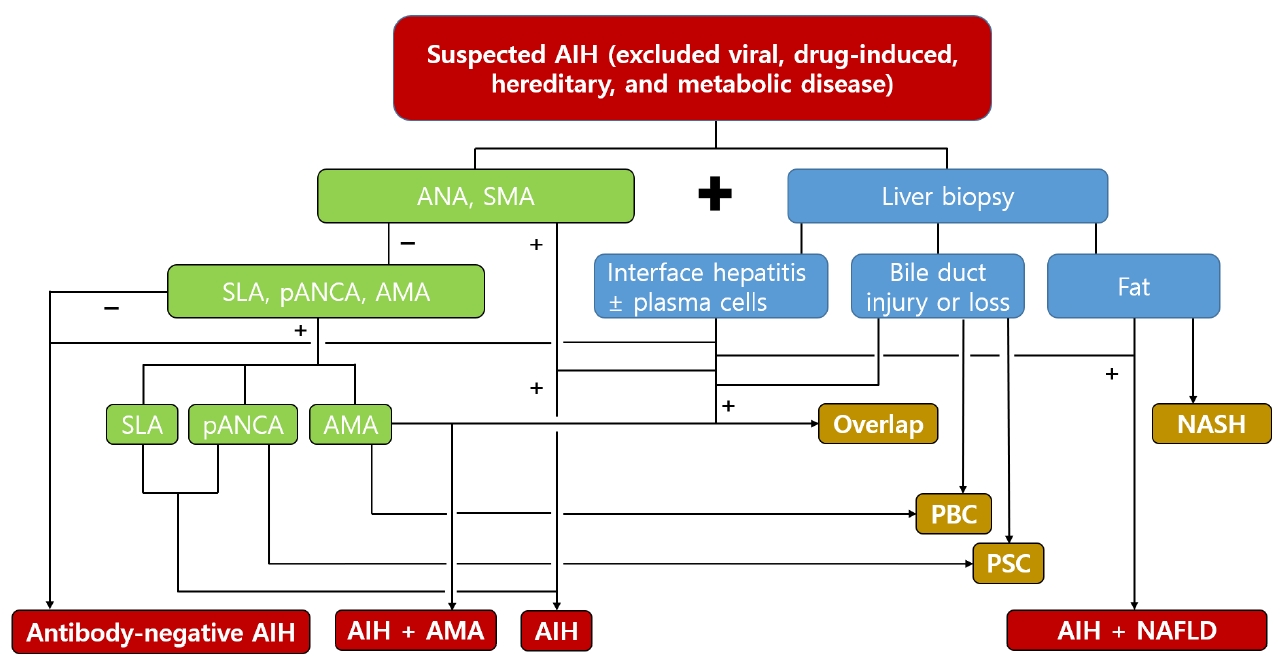
자가면역간염의 진단은 조직학적 이상(계면간염), 특징적인 임상 및 실험실 소견(증가된 혈청 AST, ALT 및 IgG) 그리고 하나 이상의 특징적인 자가항체의 존재를 기반으로 한다. 자가 면역간염은 특징적인 진단 표지자가 없고, 다른 만성 간질환의 원인(바이러스간염, 약제 유발 간 손상, 윌슨병, 유전성 혈색소 침착증 등)에 대한 배제가 필요하다(Fig. 2) [4,14,15]. 자가면역 간염에 대한 진단 기준과 진단 점수 체계는 1993년 제안되어 최근까지 개정되었고, 2015 유럽간학회 진료지침과 2019 미국간학회 진료지침에서도 언급되고 있다[3,15].
검사 결과
자가면역간염은 혈청 빌리루빈 농도와 아미노전이효소가 정상 범위보다 매우 증가되더라도 담즙정체효소는 정상 또는 미세한 상승 정도만 보이는 것이 특징적인 검사실 소견이다[4,16-18]. 다만 최근 연구에서 아미노전이효소의 상승과 함께 알칼리성 인산분해효소(alkaline phosphatase)가 아닌 감마 글루타밀전이효소(gamma glutamyl transferase)가 증가할 수도 있으며, 나아가 치료 반응의 독립적인 예측인자로 사용될 수 있음을 보고하였다[19,20].
간경변증이 동반되지 않은 자가면역간염 환자의 85%에서 혈청 IgG 증가가 확인되었으나 급성 발병 환자에서는 IgG 수치가 정상인 환자의 비율이 많았다[21,22]. 혈청 IgG가 높은 것은 자가면역간염의 특이적인 소견이며 혈청 IgA 및 IgM은 일반적으로 정상이다. 혈청 IgA와 IgM의 증가는 각각 알코올 지방간염 및 원발담즙성담관염과 같은 다른 질병이 있음을 시사한다[18].
아미노전이효소의 상승 정도는 조직학적으로 평가되는 자가면역간염의 중증도를 반영하지는 않지만, 아미노전이효소 및 면역글로불린 수치는 치료에 대한 반응과 관해 달성을 모니터링하는 데 유용한 지표로 이용된다[14].
바이러스 표지자의 부제가 자가면역간염을 진단하는 기준에 포함되지만, 바이러스간염 유병률이 높은 국가에서는 자가면역간염과 바이러스간염이 동반될 수 있다[23,24]. 이러한 경우, 명확한 진단 기준과 치료법이 정해진 바이러스간염과 비교하여 동반된 자가면역간염의 진단이 간과될 수 있기 때문에 주의가 필요하다. 자가면역간염을 치료하지 않으면 임상 증상의 악화 및 불량한 예후를 보일 수 있으므로, 임상적으로 자가면역간염이 의심될 때에는 적극적으로 혈청 학적 검사와 간 생검을 통해 동반된 자가면역간염이 있는지에 대한 평가를 고려하여야 한다.
자가항체
자가면역간염은 특정 자가항체에 따라 제1형과 제2형의두 가지 유형으로 나눌 수 있다(Table 1). 제1형은 자가면역 간염의 대부분을 차지하며 어느 연령에서나 발현하고 발견 당시 약 28% 정도에서 간경변증을 동반한다. 또한 치료에 대한 반응이 좋으나 약제 중단 시 재발의 가능성이 있다. 제2형은 주로 14세 미만의 소아에서 많이 발생하고, 급성의 임상 증상을 보이며 치료에 대한 반응이 좋지 않다. 자가항체의 경우, 제1형은 ANA 및/또는 평활근항체(smooth muscle antibody, SMA)/항액틴 항체(anti-actin antibody)를 특징으로 하고, 제2형은 대개 ANA 및 SMA의 부재와 항간신마이크로좀 1형 항체(antibody to liver kidney microsome type 1, anti-LKM1)를 특징으로 한다[25]. 이와 같이 ANA, SMA, anti-LKM-1 및 여러 자가항체는 자가면역간염 진단을 위한 중요한 지표이다[11]. ANA는 자가면역간염이 있는 북미 백인 성인의 80%에서 검출되며, SMA는 60%, anti-LKM-1은 3%에서 존재한다. 자가면역간염 환자의 49%는 진단 시 ANA, SMA 또는 anti-LKM-1를 단독 혈청학적 소견으로 보이며, 51%는 다중 항체에 대해 양성으로 확인된다[26]. 또한 특징적인 임상 소견이 동반된 자가면역간염의 최대 20%에서 ANA, SMA, anti-LKM-1 음성인 경우가 존재하므로, 혈청 음성 자가면역간염이 의심된다면 다른 자가 항체를 확인해 보아야 한다(Fig. 2). 알려진 다른 자가면역항체로는 perinuclear anti-neutrophil cytoplasmic antibodies (pANCA), liver specific cytosol antigen type 1 (anti-LC1), antibodies to asialoglycoprotein receptor (anti-ASGPR), IgA endomysial antibodies, antibodies to soluble liver antigen/liver pancreas (anti-SLA/LP), anti-actin 등이 있다(Table 2) [10,11,15]. 자가면역항체는 질병 특이적이 아니며 질병의 경과 중 변화할 수 있으므로, 한 번의 검사에서 자가항체 역가가 낮다고 자가면역간염을 배제하지 못한다. 또한 동반된 임상 소견이 없음에도 불구하고 항체 역가가 높다는 것만으로 자가면역간염을 진단 내릴 수 없다. 성인과 소아 모두에서 자가항체 역가가 질환의 진단 및 질병의 중등도와 치료 반응을 대략적으로 반영하지만, 질병의 경과나 예후에 대한 확립된 표지자는 아니다[27-30].
조직학적 특징
자가면역간염은 간 생검과 합당한 조직학적 소견 없이는 진단될 수 없다. 계면간염은 자가면역간염의 특징적인 조직학적 소견이며 66%에서 형질세포 침윤, 47%에서 소엽간염 (lobular hepatitis)이 동반된다. 중심소엽괴사(centrilobular necrosis)는 간경변증 동반 여부와 상관없이 29%에서 발견된다[31,32]. 또한 emperipolesis (active penetration by one cell into and through a large cell)는 65%의 자가면역간염에서 확인되며, rosettes는 33%에서 나타난다. 개별 조직학적 소견 중자가면역간염에 특이적인 소견은 없으나, 소엽으로 확장되는 문맥 림프구성 또는 림프형질구성 세포와의 계면 간염 소견, emperipolesis 및 rosettes 소견은 자가면역간염의 전형으로 간주된다[33]. 진단 시 조직학적 소견은 다른 간질환에 대한 진단을 배제하고, 염증 활성도의 중증도를 등급화하고 섬유화 정도를 나타내기 위해 필수적이다[34-36].
진단 점수 기준
자가면역간염의 전형적인 사례 외에 비전형적인 사례의 진단을 돕고, 진단을 정량화하여 객관적인 비교가 가능하도록 1993년에 IAIHG에 의해 점수제 진단이 고안되었고, 1999년수정 후 2008년에 간소화되었다(Tables 3, 4) [17,18]. 수정된 진단 점수 체계는 복잡하거나 특이한 특징을 가진 환자에게 선호되고, 간소화된 진단 점수 체계는 전형적인 환자에게 가장 정확하다. 간소화된 진단 점수 체계로 산정된 점수가 낮을수록, 수정된 진단 점수 체계로 재평가를 고려해야 한다[37]. 이러한 진단 점수 체계는 다른 원인으로 인한 간질환과 자가면역간염을 구별하는 데 매우 유용하며, 1) 자가면역 질환과의 연관성을 고려하여 자가면역 질환의 동반 여부, 2) 특정 HLA 표현형(DR3 or DR4), 3) pANCA 등과 같은 드문 자가항체 존재 유무와 함께 4) 치료 반응 및 재발 여부도 진단 항목에 반영된다. 또한 약제 복용 및 바이러스간염, 담즙 정체 질환, 알코올 간질환 등 타 질환의 감별을 도모하기 위한 항목들이 포함되어 있다. 이상과 같은 13개의 항목에 대한 점수를 더하여 치료 전 점수가 10-15점이면 가능성(probable), 16점 이상이면 확정적(definite) 진단을 내리며, 치료 후에는 각각 12-17점, 18점 이상이 필요하다[4]. IAIHG 점수 체계는 원인이 명확한 간질환과 자가면역간염을 구별하는 데 매우 유용하지만 전향적 연구를 통한 검증 부족, 동반된 간질환 (원발경화담관염, 원발담즙성담관염, 비알코올 지방간질환, 간이식, 전격성 간부전)에서의 정확성 부족, 다른 혈청학적 표지자가 제외된 점, 간접 면역 형광법에 의한 자가항체 측정과 같은 제한점 역시 존재한다[38,39].
자가면역간염의 치료
자가면역간염이 진단되면 치료를 고려해야 한다. 만약 치료하지 않으면 5년 및 10년 생존율이 50%와 10%에 불가할 정도로 예후가 불량하며, 심한 자가면역간염의 경우 6개월내 40%가 사망하며, 생존자 중 최소 40%가 간경변증으로 진행할 수 있다[40]. 하지만 면역억제제 등 적절한 치료를 할 경우 10년 생존율은 80-93%로 향상된다[41]. 자가면역간염에서 1차 요법의 목적은 약물 유발 합병증을 최소화하면서 증상을 개선하며, 간 내 염증을 조절하고 생화학적 관해 달성 및 추가적인 간질환의 진행을 예방하고 간 섬유화를 호전시키는 것이다. 이상적인 생화학적 관해 달성은 혈청 아미노전 이효소 및 IgG의 정상화이며, 비활동성 질환을 제외한 모든 자가면역간염 환자는 치료 대상이 될 수 있다[42,43]. 표준치료로 프레드니솔론 단독 또는 아자치오프린 병합요법을 고려할 수 있다. 아자치오프린의 경우 thiopurine methyltransferase (TPMT) genotyping을 통해 thiopurine methyltransferase의 결핍이 없는 것이 확인되면 프레드니솔론 치료 시작 2주 뒤 추가할 수 있다. 중증 급성 질환의 경우에는 고용량 프레드니솔론 단독으로 치료를 시작하고, 치료 시작 2주 후에 혈청 빌리루빈이 6 mg/dL 이하로 떨어지면 TPMT genotyping을 확인 후 아자티오프린을 추가할 수 있다[44].
결론
자가면역간염은 최근 점차 늘어나는 추세로, 이에 대한 진단의 중요성이 강조되고 있다. 자가면역간염의 진단은 우선 다른 만성 간질환에 대한 원인 배제가 필요하며, 특징적인 진단 표지자가 없기 때문에 급성이나 만성 간질환 환자에서 감마글로불린이 증가되어 있는 경우 자가항체를 검사함으로써 의심해볼 수 있다. 최근 자가면역성간염 및 원발담즙성담 관염이 의심되지만 ANA, AMA, SMA가 모두 음성인 경우 IgG 자가항체 4종(SLA/LP, LC-1, LKM-1, AMA-M2)을 추가로 시행할 수 있게 급여 기준이 변경되었으므로, 이와 같은 검사를 이용하는 것도 진단에 도움이 될 수 있다. 임상적으로 자가면역간염이 의심될 경우 간 생검은 자가면역간염의 진단에 필수적인 요소가 되고, 특징적인 조직학적 소견이 있을 경우 확정적으로 진단할 수 있다. 본고에서 기술한 바와 같이 자가면역간염의 임상 소견을 잘 이해하고 정확한 진단을 위해 적극적인 검사를 한다면 적절한 치료를 통해 환자의 예후를 호전시키는 것을 기대할 수 있겠다.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






