카바페넴 내성 장내세균에서의 새로운 베타락탐/베타락타마제 억제제 병합 항균제의 감수성 평가와 고찰
Susceptibility Assessment and Review of Novel Beta-Lactam/Beta-Lactamase Inhibitor against Carbapenem-Resistant Enterobacterales
Article information
Abstract
목적
카바페넴 내성 장내세균속(carbapenem-resistant Enterobacterales, CRE)에 의한 감염은 낮은 항균제 감수성률, 치료제의 부작용으로 인한 높은 사망률, 제한된 치료 옵션 등으로 인하여 전 세계적으로 중대한 공중보건 위협으로 간주된다. 최근 도입된 베타락탐/베타락타마제억제제병합제(β-lactam/β-lactamase inhibitors, BLBLIs)는 특정 카바페넴분해효소(carbapenemase) 생성 CRE에 대한 1차 치료제로 활용되고 있다. 본 연구는 국내 CRE 균주를 대상으로 BLBLIs에 대한 감수성을 평가하고 항균제 관리 최적화 및 내성 감시의 중요성을 강조하고자 하였다.
방법
Imipenem 최소 억제 농도 측정 및 imipenem, meropenem, ertapenem에 대한 디스크 확산법을 통해 총 71 주의 CRE 균주를 선별하였다. 모든 CRE 균주에 대해 ceftazidime-avibactam, imipenem-relebactam, meropenem-vaborbactam의 감수성 검사를 시행하였고 동시에 카바페넴분해효소 유전형 분석을 수행하였다.
결과
총 71주의 CRE 균주 중 KPC 생성 균주는 46주, NDM형은 10주, OXA-48-like형은 2주였으며 나머지 13주는 카바페넴분해효소 비생성(non-CP) CRE로 확인되었다. 전체 CRE 균주에 대한 ceftazidime-avibactam, imipenem-relebactam, meropenem-vaborbactam의 감수성률은 각각 84.5%, 80.3%, 83.1%였다. KPC 생성 균주에 대해서는 세 약제 각각 97.8%, 93.5%, 95.7%의 높은 감수성률을 보였다.
결론
새로운 BLBLIs는 국내 CRE 균주에 대해 전반적으로 높은 감수성률을 보였으며 특히 KPC 생성 균주에서는 90% 이상의 감수성을 보였다. 이러한 결과는 CRE 감염 치료에서 BLBLIs의 임상적 유용성을 뒷받침하며 내성 균주의 조기 발견과 확산 방지를 위한 지속적인 감시 체계 구축이 필요함을 시사한다.
Trans Abstract
Background/Aims
Carbapenem-resistant Enterobacterales (CRE) infections represent a significant global health concern, characterized by low susceptibility rate- and adverse effect-related high mortality and limited treatment options. Novel beta-lactam/beta-lactamase inhibitors (BLBLIs) are first-line therapeutic agents against specific carbapenemase (CP)-producing CREs. We assessed current CRE susceptibility to these novel BLBLIs to aid optimal antimicrobial stewardship, emphasizing the need for continuous resistance surveillance.
Methods
In total, we identified 71 CRE isolates based on the imipenem minimum inhibitory concentration and disk diffusion susceptibility testing for imipenem, meropenem, and ertapenem. We performed antimicrobial susceptibility testing for novel BLBLIs, including ceftazidime-avibactam, imipenem-relebactam, and meropenem-vaborbactam as well as CP gene molecular characterization for all CRE isolates.
Results
We analysed a total of 71 CRE isolates and our CP genotypic analysis identified 46 Klebsiella pneumoniae CP (KPC)-producing, 10 New Delhi metallo-beta-lactamase-producing, and two oxacillinase-48-like producing isolates. We identified the remaining 13 isolates as non-CP-producing CREs. The susceptibility rates for ceftazidime-avibactam, imipenem-relebactam, and meropenem-vaborbactam were 84.5%, 80.3%, and 83.1%, respectively. Among the CP-producing isolates, KPC producers exhibited susceptibility rates of 97.8%, 93.5%, and 95.7% to ceftazidime-avibactam, imipenem-relebactam, and meropenem-vaborbactam, respectively.
Conclusions
Novel BLBLIs generally yielded high CRE susceptibility rates, with the latter exceeding 90% in KPC-producing isolates. Although these findings indicate the efficacy of novel BLBLIs in treating CRE infections, ongoing surveillance is essential to detect and mitigate resistant strain emergence.
INTRODUCTION
Carbapenems, including imipenem, ertapenem, meropenem, and doripenem, were once considered the last resort for treating multidrug-resistant Gram-negative bacteria also resistant to broad-spectrum beta-lactams. However, following the development of imipenem in 1985, the first carbapenemase enzyme-producing Klebsiella pneumoniae was detected in 1996 and since then, carbapenem-resistant Enterobacterales (CRE) have been rapidly increasing worldwide. In Korea, since surveillance system expansion to nationwide monitoring in 2017, the number of CRE cases reported through the Korea Disease Control and Prevention Agency’s Disease Health Management System has been continuously increasing. In 2024, a total of 42,347 cases (i.e., 2,747 patients and 39,600 carriers) were reported across the country [1]. CRE can be broadly classified into two resistance mechanism-based types: carbapenemase-producing Enterobacterales (CPE), which produce carbapenemase enzymes that directly degrade carbapenems, and non-carbapenemase-producing CRE, which acquire resistance through further mechanisms like the combination of AmpC β-lactamase production and porin loss without producing carbapenemase. Approximately 71% of CRE cases documented in Korea reportedly belong to the CPE category, and 83% of the CRE cases were reported as CPE in the United States [2,3]. Carbapenemases are classified into four classes based on their amino acid sequences, including Ambler class A (K. pneumoniae carbapenemase, KPC), C, and D (oxacillinases, OXA), which require a serine residue for their activity, and Ambler class B (New Delhi metallo-β-lactamases [NDM], imipenemase metallo-β-lactamases [IMP], Verona integron-encoded metallo-β-lactamase [VIM]), which requires zinc for its activity. While the CRE-produced carbapenemase types vary by region, approximately 77-80% of CPE cases in Korea and the United states reportedly produce KPC of ambler class A.
CRE treatment options remain significantly limited. Recently developed β-lactam/β-lactamase inhibitor combinations (BLBLIs) are highly effective against KPC-producing CRE. In Korea, the BLBLIs ceftazidime-avibactam has been introduced and is currently used, susceptibility testing for them is thus crucial for guiding treatment decisions and monitoring the emergence of new resistance. In this study, we aimed to investigate the susceptibility rates of CRE isolates from our institution to BLBLIs and other antimicrobial agents commonly used for CRE infection treatment.
MATERIALS AND METHODS
From August 2024 to January 2025, the susceptibility rates of β-lactam/β-lactamase inhibitors and other antimicrobial agents were analyzed for CRE isolates collected from the laboratory. The strains were collected based on the minimum inhibitory concentration results obtained using the VITEK® 2 system (bioMérieux, Marcy l’Etoile, France). CRE strains were defined as resistant to at least either imipenem or ertapenem according to the results of the antimicrobial susceptibility test conducted with the AST-N413 card (bioMérieux). In addition, disc diffusion testing with imipenem, meropenem, and ertapenem was performed, and resistance was confirmed according to the Clinical and Laboratory Standards Institute (CLSI) guideline M100, ED34 [4] interpretative criteria. CRE strains were tested for susceptibility to BLBLIs and other antimicrobial agents using the AST-N439 card (bioMérieux), and the susceptibility rates were analyzed based on the results. Furthermore, non-CP-CRE and CP-CRE were identified using the modified carbapenem inactivation method (mCIM). For all mCIM-positive isolates, carbapenemase subtype phenotypic testing was performed using the NG-Test® CARBA5 (NG Biotech, Guipry-Messac, France), which can detect and differentiate five major carbapenemase subtypes: KPC, NDM, IMP, VIM, and OXA-48-like enzymes. In addition, for isolates submitted to the Korea Health Environmental Institute for surveillance purposes, CPE result consistency from the institute was confirmed. In the Korea Health Environmental Institute, carbapenemase genes (KPC, NDM, OXA, IMP, VIM, Guiana extended spectrum β-lactamase [GES], Sang Paulo metallo-β-lactamase [SPM], German imipenemase [GIM], Seoul imipenemase [SIM], and Serratia marcescens enzymes [SME]) were identified using qualitative polymerase chain reaction, and, when necessary, specific genotypes were determined using sequencing. Supplementary sequencing- based molecular characterization was not carried out in our institution. The susceptibility rates for imipenem-relebactam, ceftazidime-avibactam, meropenem-vaborbactam, tigecycline, and fosfomycin were analyzed according to the carbapenemase enzyme phenotype. This study was approved by the Institutional Review Board (HPIRB NON2024-001-001).
RESULTS
In total, 71 CRE isolates were analyzed, including 54 K. pneumoniae, nine Escherichia coli , three Enterobacter spp., one Serratia marcescens, one Citrobacter freundii , one Citrobacter braakii , and one Enterobacter cloacae. Among these, carbapenemase (CP) gene typing revealed that 46 isolates were KPC producers, 10 isolates harbored NDM, and 2 isolates produced OXA-48-like. The remaining 13 isolates did not carry any CP genes and were classified as non-CP-producing CREs (Fig. 1).
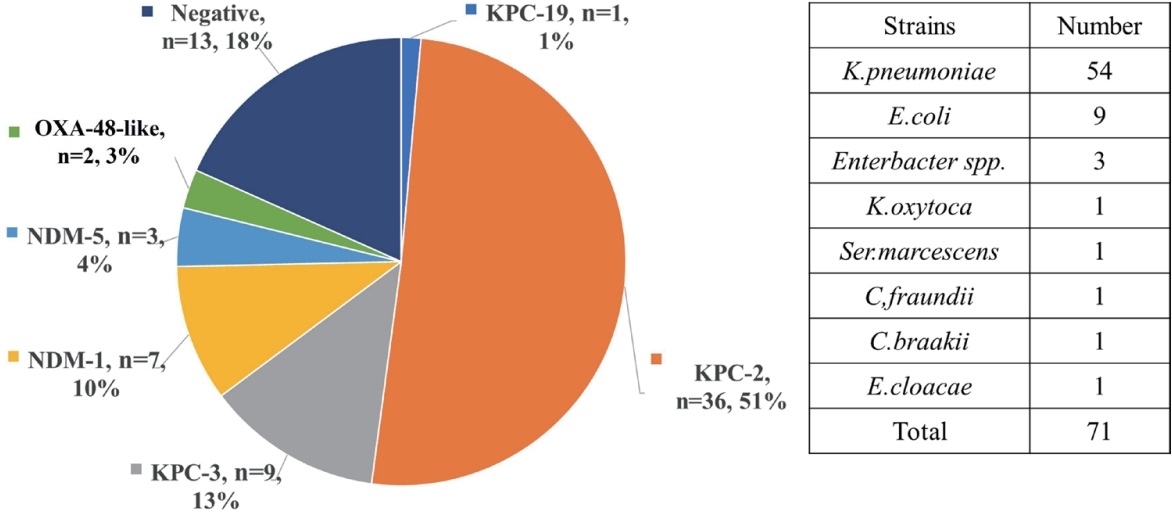
The types of strains included in this study and carbapenemase gene distributions. KPC, Klebsiella pneumoniae carbapenemase; OXA, oxacillinase; NDM, New Delhi metallo-β-lactamases.
The overall susceptibility rates of the 71 CRE isolates to ceftazidime- avibactam, imipenem-relebactam, and meropenem- vaborbactam were 84.5%, 80.3%, and 83.1%, respectively (Table 1). Among the CP-producing isolates, KPC-producing isolates demonstrated high susceptibility, with rates of 97.8%, 93.5%, and 95.7% to ceftazidime-avibactam, imipenem-relebactam, and meropenem-vaborbactam, respectively. All non-CP-producing CRE isolates exhibited complete susceptibility (100%) to both ceftazidime-avibactam and imipenem-relebactam. One non-CP-producing CRE isolate exhibited intermediate to meropenem-vaborbactam. Similarly, OXA-48-like-producing isolates also displayed 100% susceptibility to ceftazidime-avibactam and meropenem-vaborbactam. One OXA-48-like-producing isolate revealed imipenem-relebactam resistance. In contrast, NDM-producing isolates exhibited 100% resistance to ceftazidime–avibactam, imipenem-relebactam, and one isolate exhibited susceptibility to meropenem-vaborbactam. Furthermore, CRE isolates retained susceptibility rates of 77.5% and 83.1% to tigecycline and fosfomycin, respectively. KPC-producing CRE susceptibility to tigecycline and fosfomycin was 82.6% and 84.8%, respectively.

CRE antimicrobial susceptibility rate to BLBLIs
DISCUSSION
In this study, we aimed to evaluate the susceptibility rates of newly developed and clinically used BLBLIs, including ceftazidime-avibactam. Among KPC-producing CRE, which represent the primary target pathogens for these agents, the susceptibility rates to ceftazidime-avibactam, imipenem-relebactam, and meropenem-vaborbactam were 97.8%, 93.5%, and 95.7%, respectively. A recent Korean study described similar results, with 184 out of 186 KPC-2-producing isolates (98.9%) susceptible to ceftazidime-avibactam, 173 (93.0%) to imipenem-relebactam, and 184 (98.9%) to meropenem-vaborbactam [5]. According to data reported from other countries, ceftazidime-avibactam demonstrated high in vitro activity, with 99.3% susceptibility against KPC-2-, OXA-48-like-, and imipenemase (IMI)-producing isolates, and 91.4% susceptibility among non-CP-CRE. As expected, no activity was observed against metallo-β-lactamase (MBL)- or IMP-producing isolates [6]. Moreover, a domestic study first reported the acquired ceftazidime-avibactam resistance emergence during treatment in K. pneumoniae, underscoring the critical need for epidemiological monitoring and surveillance [7]. Similar resistance emergence trends upon ceftazidime-avibactam treatment have also been documented internationally [8]. Therefore, routine susceptibility testing for these new BLBLIs, still not widely implemented in a lot of clinical laboratories, should be prioritized to support appropriate antimicrobial stewardship.
Currently, various clinical studies are underway to develop new treatment options against CRE infections. For this purpose, certain antibiotics, although not yet introduced in Korea, have been approved and are currently in use in the United States and Europe. The CRE treatment strategy recommended by the Infectious Diseases Society of America (IDSA) involves using standard-spectrum antibiotics for which susceptibility has been confirmed through antimicrobial susceptibility testing. However, if resistance is identified against all standard-spectrum antibiotics, including carbapenems, treatment recommendations are based on CRE-produced carbapenemase enzyme presence and type [9]. In particular, for KPC-type carbapenemase, prevalent in Korea, the recommended treatment includes BLBLIs, such as ceftazidime-avibactam, meropenem-vaborbactam, and imipenem-relebactam. Alternative antibiotics include cefiderocol, tigecycline, and eravacycline (the latter two for intra-abdominal infections).
Unlike classic β-lactamase inhibitors, acting as suicide substrates by sharing the β-lactam ring structure, recently developed BLBLIs (e.g., avibactam, durlobactam, relebactam, and vaborbactam) inhibit β-lactamases by forming covalent bonds with the serine residues in the active sites of the enzymes. Consequently, these inhibitors display their activity against serine beta-lactamases (e.g., KPC and OXA), whereas metallo-β-lactamases (e.g., NDM, VIM, and IMP) are known to be resistant to these agents. In this study, KPC-producing isolates exhibited a very high susceptibility rate of 93.5-97.8% to all three BLBLIs, whereas NDM-producing isolates remained mostly resistant. Although OXA-type CREs were expected to be susceptible, the small number of isolates included in this study made drawing definitive conclusions difficult. Therefore, although KPC-producer resistance to BLBLIs observed in this study could be attributed to a major error in testing or mutation, further testing with the E-test revealed susceptibility, suggesting a potentially major error in the initial testing. In addition, although NDM-producing strains might be susceptible to meropenem-vaborbactam, these agents are presumably not active in vitro, thereby potentially necessitating BLBLIs with aztreonam.
Ceftazidime-avibactam is second-generation BLBLIs, which was approved in the United States in 2015. In Korea, it was launched as a non-reimbursed drug in July 2023 and has been included in the national health insurance reimbursement list since March 2024. Ceftazidime-avibactam can be used in cases when carbapenem antibiotics have failed, including complex intra-abdominal and urinary tract infections, hospital-acquired pneumonia, including ventilator-associated pneumonia, as well as in cases involving confirmed multidrug-resistant Pseudomonas aeruginosa or CRE. Therefore, ceftazidime-avibactam use is anticipated to increase in the future, and with this in mind, the importance of antimicrobial susceptibility testing has also come to the forefront. Although ceftazidime-avibactam application has not yet become widespread in Korea, KPC-type CREs have already been detected at very high levels. Therefore, data review of the appropriate ceftazidime-avibactam use and the corresponding resistance rates is required. According to an analysis by Wang et al., [10] Enterobacteriaceae demonstrate a notably low resistance to ceftazidime-avibactam with an overall resistance rate below 0.6%. P. aeruginosa exhibits lower susceptibility to ceftazidime-avibactam, with reported resistant rates ranging from 2.9% to 18.0%. In Acinetobacter baumannii , ceftazidime-avibactam resistance exceeds 50%. The European Centers for Disease Control and Prevention (CDC) has highlighted the risk of resistance to ceftazidime-avibactam in CRE, and capacity and method enhancement of clinical microbiology laboratories for ceftazidime-avibactam resistance detection as well as epidemiological surveillance improvement is recommended to mitigate this risk [11]. In addition, based on data from the 2023 national antimicrobial resistance surveillance report in Korea [12], the KPC-producing K. pneumoniae resistance rate to ceftazidime-avibactam was 5.5%. Therefore, monitoring the current ceftazidime-avibactam resistance rates in Korea as well as those of other newly developed BLBLIs is important.
While BLBLIs response can be estimated based on the isolated CPE types by different institutions, it is crucial to note that new BLBLIs exhibit resistance or susceptibility patterns specific to certain CRE types. Therefore, for the efficient use of these agents, conduct tests to identify the CP type is imperative. Furthermore, even though BLBLIs currently yield high susceptibility rates, continuous surveillance is necessary to monitor the emergence of new resistance mechanisms. To support this, clinical microbiology laboratories should display the capacity to perform BLBI susceptibility testing.
Notes
CONFLICTS OF INTEREST
No potential conflicts of interest relevant to this article were reported.
FUNDING
This study was supported by a research grant from Inje University Haeundae Paik Hospital.
AUTHOR CONTRIBUTIONS
The author confirms sole responsibility for the following: study conception and design, data collection, analysis and interpretation of results, and manuscript preparation.
ACKNOWLEDGEMENTS
This study was supported by Inje University Haeundae Paik Hospital.